What Research in a Hospital Taught Me About Designing Educational Products in Healthcare
Estimated reading time: 6 minutes
I The Beginning
I began my healthcare design journey eight years ago in my hometown. Today, working within the UK healthcare system, I can trace much of my systems thinking back to that first encounter.
At that time, there were very few thoughtfully designed educational products for children with autism where I lived. I chose this as the topic of my final project for my BFA in Product Design.
I still remember the first day I walked into a special school. I was excited for my first research study. But I was also nervous and scared.
I wasn’t sure whether I was capable of completing such a complex project within a year by myself. Too sensitive, too important. But I went in anyway.
I embedded myself in the school environment for several months as a volunteer researcher. Each volunteer was paired with one child. We sat at the back of the classroom, assisting when needed. We played games. We ran to the playground to fetch balls. They looked just like any other children.
And I remember thinking:
‘Maybe they’re just normal kids, we all went through that time.‘
But that was an arrogant thought.
Design school taught me methods and tools, but conducting user research with autistic children requires far more than design frameworks. It requires patience, humility, and unlearning.
II Observations to Insights, Insights to Product Principles
Later, I volunteered in a larger organisation for children with special educational needs, which had a wide range of sensory toys to support the development of the five senses.
I followed what I had been taught. Observe first. Collect first-hand material. Watch how your target audience behaves. Understand their habits and needs. Notice how they react in different situations. Then speak with stakeholders who can deepen your understanding: Parents, teachers, therapists.
I immersed myself in parents’ chat groups and volunteer communities, thinking about how we could design something meaningful to support families. That is the core of design, especially in healthcare: truly knowing your users.
I wrote down what I saw.
Then I returned to the studio to summarise and conduct second-hand research.
‘Target User A was suddenly screaming during transitions.’
‘Target User B was suddenly crying quietly in the middle of the session.’
‘All children focused longer in music class than in other structured learning tasks.’
I mapped what they did, how they reacted, what each class was trying to achieve, and how teachers measured progress. I created a user journey map based on these observations.
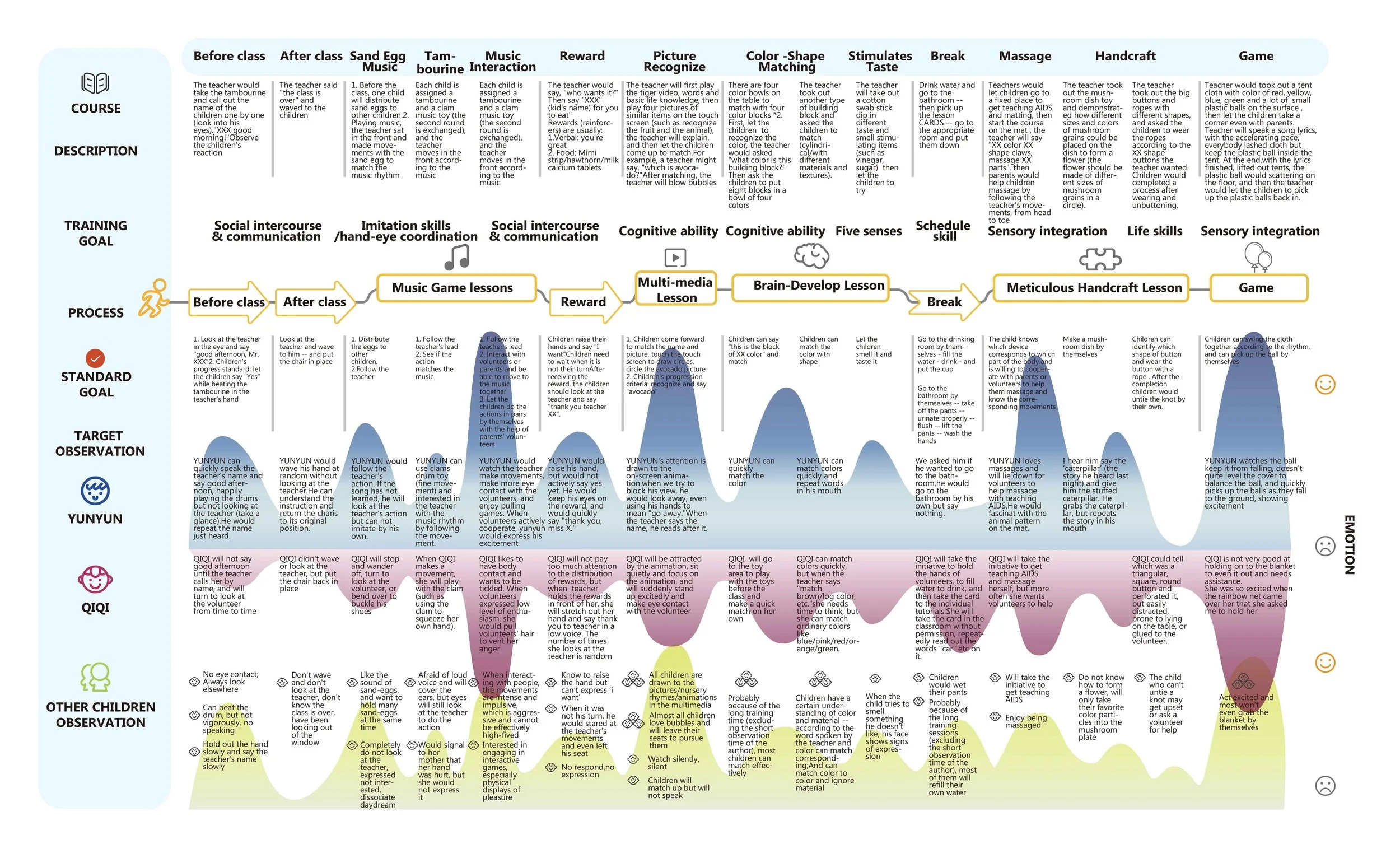
User Journey Map. Zhai,C., Chen,X.(2022).Design of Rehabilitation-assisted Interactive Toys for Children with Autism.
I documented behaviour patterns without interpretation, separating observable actions from assumed meaning. When I began translating observations into insights, I encountered the limits of surface-level research.
‘Children pay more attention during music class... maybe I can use it as a portal, an attractive starting point to embed learning methods.’ I realised I was reacting at the feature level.
Add music. Add sound. Add stimulation.
But why music? Why only music? What about light? What about touch?
Why?
‘Child screams suddenly during the transition between activities.’ That was one of my notes.
What uncertainty triggered the behaviour? What internal state changed? What regulation mechanism was activated?
‘Transitions create anxiety because predictability collapses. Different children respond differently. Predictable rhythm may reduce cognitive load and create a sense of safety.’
I think that is the underlying mechanism.
And that is where design shifts from adding more features to defining principles:
‘Make transitions predictable and visible before they happen’ > ‘Use rhythm as a form of regulation’; ‘Provide multi-sensory cues before shifts occur’ > ‘Reduce sudden changes’...
This was the turning point in how I think about healthcare product development. These principles can then be broken down into Why > How > What.
Why clarifies priorities.
How opens space for multiple possible solutions.
What becomes the tangible design outcome.
III What am I really designing for?
‘What we feel affects how we think and act; what we do affects how we think and feel; What we think affects how we feel and act.’
It’s a CBT (Cognitive Behavioural Therapy)looping triangle. A system.
Before designing, we need to dig deeper to understand the regulation.
At that time, I was overly focused on attention.
‘Which classes attracted the most attention? Which tools kept children engaged? ‘
I began searching for a setting that best aligned with children’s natural tendencies, trying to embed learning into toy design.
Then I realised I had drifted toward the wrong optimisation metric.
‘Emotional Safety ’, ’ Self-regulation ’, ’ Reduced stress markers’’parent relief’...
Identifying what is essential, what is a priority, and what is just nice-to-have is critical in healthcare design. It forces you to define the invisible variable. What are you truly designing for?
IV From Product Thinking to System Thinking
Living and working within two different healthcare contexts has shown me how differently autism is perceived, diagnosed, and supported culturally. Clinical criteria, public awareness, and structural support systems vary significantly across regions.
Autism cannot be approached as a homogeneous user segment. It reflects a spectrum of nervous system regulation patterns.
Instead of designing a ‘Product for autistic children‘, we need more focused definitions of who we are supporting: sensory-seeking children, sensory-avoidant children, verbal-limited communicators, and parents under chronic stress.
Clarifying who we are designing for narrows the problem space and guides product direction.
Healthcare design is never just about a product. It is a multi-layered system shaped by clinical structures, education systems, family dynamics, policy, and culture. It requires collaboration across departments and disciplines.
That early research shaped how I approach every educational healthcare design project today.
VI. A Recent Small Conversation
Recently, near the end of a workday in the hospital, I was chatting with one of our cleaners. She told me both her grandchildren are autistic.
One of them did not speak much when he was young, she said. He loved maths.
He now works at the local council.
Stories like this remind me why I entered healthcare design in the first place.
In Chinese, we sometimes call autistic children ‘星星的孩子’. It means children of the stars.
I know design cannot solve everything. But shaping safer, more responsive systems, with care and intention, is one way to help people shine in their own world, in their own way, like stars.
That belief now guides how I design and develop educational learning experiences within complex hospital systems.
-
-
Online course Design in Healthcare: Using Patient Journey Mappingfrom TU Delft.
Book - Delft Design Guide - offers an overview of the perspectives, models, approaches, and methods embedded in the Industrial Design study programs.
I’m always interested in learning from others in healthcare XR & Design. If you’re working on similar projects, let’s connect!
Follow me on LinkedIn